Beyond Observance: Why World Nutrition Day Demands a Strategic Rethink
World Nutrition Day, observed each year on 28 May, typically triggers a wave of social media campaigns, infographic-heavy awareness drives, and short-lived news coverage of malnutrition statistics. The conversation turns to statistics: how many children are malnourished, how many women are anaemic, how far the world is from its 2030 targets. For organisations active in the social sector, that is not enough. The day must demand something more rigorous – an honest examination of whether nutrition interventions are actually producing the outcomes they were designed to achieve.
For development organisations, foundations, NGOs, and public health teams, the key question is no longer how many beneficiaries were reached or how many nutrition sessions were conducted. The more important question is: what changed? Did dietary diversity improve? Did anaemia decline? Did infant feeding practices change sustainably? Did households adopt healthier nutrition behaviours over time? That is the difference between an activity-led programme and an outcome-driven nutrition intervention.
“The strongest nutrition programmes are not the ones that do the most activities. They are the ones that can show what changed, for whom, why it changed and how that change can last.”
Across South Asia, Sub-Saharan Africa, and much of the Global South, decades of investment in nutrition programming have expanded coverage and reach considerably. Supplementary nutrition, iron–folic acid distribution, and growth-monitoring activities now operate at enormous scale. Yet the gap between what is delivered and what changes in people’s lives remains wide– and often unexamined. The next generation of nutrition programme design must be explicitly outcome-driven: rooted in evidence, structured around a clear theory of change, tracked through robust monitoring evaluation and learning (MEL) frameworks, and designed from the outset for sustainability.
The Global Nutrition Challenge: Scale, Persistence, and Regional Disparity
The 2025 UNICEF–WHO–World Bank Joint Child Malnutrition Estimates present a sobering global picture. In 2024, an estimated 150.2 million children under five were stunted– down from 180.4 million in 2012, but far short of the 2030 SDG target 2.2 to end all forms of malnutrition. Some 42.8 million children were wasted (6.6% prevalence), 12.2 million of them severely. Another 35.5 million were overweight. Only 28% of countries are on track to halve stunting by 2030, and just 17% are expected to meet the child overweight target.
Anaemia remains among the most persistent and under-addressed nutrition challenges worldwide. WHO estimates that approximately 571 million women aged 15–49 and 269 million children aged 6–59 months were anaemic globally in 2019– with the African and South-East Asia regions carrying over 60% of the burden. Anaemia prevalence among women of reproductive age has barely declined since 2000, even as stunting has slowly improved. That stagnation is not accidental; it reflects inadequate programme design, poor adherence mechanisms, and persistent gaps in behaviour change.
The economics are equally stark. The World Bank estimates that undernutrition and micronutrient deficiencies cost the global economy at least $3.5 trillion annually. Its 2024 Investment Framework for Nutrition calculates that scaling up evidence-based interventions could prevent 6.2 million child deaths and avert 27 million stunting cases over 2025–2034, generating $2.4 trillion in economic benefits– a return of approximately $23 for every $1 invested. The cost of continued inaction: an estimated $41 trillion over the same period.
Regionally, the burden is deeply unequal. South Asia and Sub-Saharan Africa together account for over 90% of the world’s stunted children. In Africa, the number of stunted children rose by over 2 million between 2012 and 2024. Within these regions, sub-national disparities are enormous: national averages mask pockets of severe deprivation where child malnutrition exceeds 45%, often concentrated in indigenous, tribal, pastoral, or conflict-affected communities.
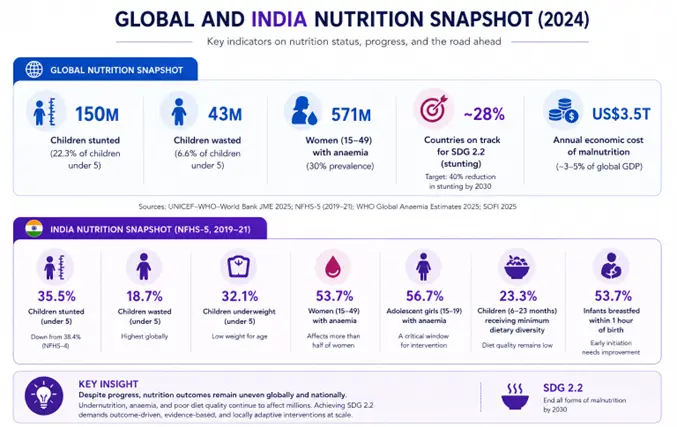
Figure 1: Key nutrition indicators– Global and India. Sources: UNICEF–WHO–WB JME 2025; NFHS-5 (2019–21); WHO Global Anaemia Estimates 2025; SOFI 2025; World Bank Investment Framework for Nutrition 2024.
India: A Microcosm of the Global Challenge
India illustrates many of these dynamics at unmatched scale. NFHS-5 (2019–21) recorded a decline in child stunting from 38.4% (NFHS-4) to 35.5%. Yet approximately 67% of children under five remain anaemic. More than half of women of reproductive age– 53.7%, or 203 million women– are anaemic (NFHS-5). The 2025 UN SOFI report placed India’s under-five wasting at 18.7%, the highest globally, affecting over 21 million children.
India’s policy response– POSHAN Abhiyaan, now integrated into Mission Poshan 2.0– has introduced convergence, digital monitoring through the Poshan Tracker (covering nearly 14 lakh Anganwadi centres and 8.95 crore beneficiaries as of March 2026), and frontline worker engagement. Similar large-scale architecture exists in Ethiopia’s Seqota Declaration, Bangladesh’s National Nutrition Services, and Nigeria’s National Multi-Sectoral Plan of Action for Food and Nutrition. But across all these contexts, the critical question is the same: are activities translating into measurable, sustained nutritional improvement?
The Output Trap: Why Output-Focused Programmes Underperform
A recurring pattern across nutrition programme evaluations– in India, East Africa, and South-East Asia– is the dominance of output measurement. Programmes track beneficiaries enrolled, meals distributed, health sessions conducted, and supplements delivered. These are necessary operational metrics, but they are not evidence that nutritional status, dietary behaviour, or health outcomes have changed.
Programme evaluations frequently show coverage targets met while outcome indicators remain flat. Supplementary nutrition reaches households, but dietary diversity does not improve. Iron tablets are distributed, but anaemia prevalence does not decline at the expected rate. Growth monitoring sessions take place, but referral pathways for severely malnourished children remain under-utilised.
This is the “output trap”: a design and measurement architecture that rewards activity over change. It persists because outputs are easier to count, faster to report, and less politically uncomfortable than honest outcome data– but it has real costs. Resources are allocated to programmes that appear successful on paper while actual nutrition impact measurement remains weak or absent.
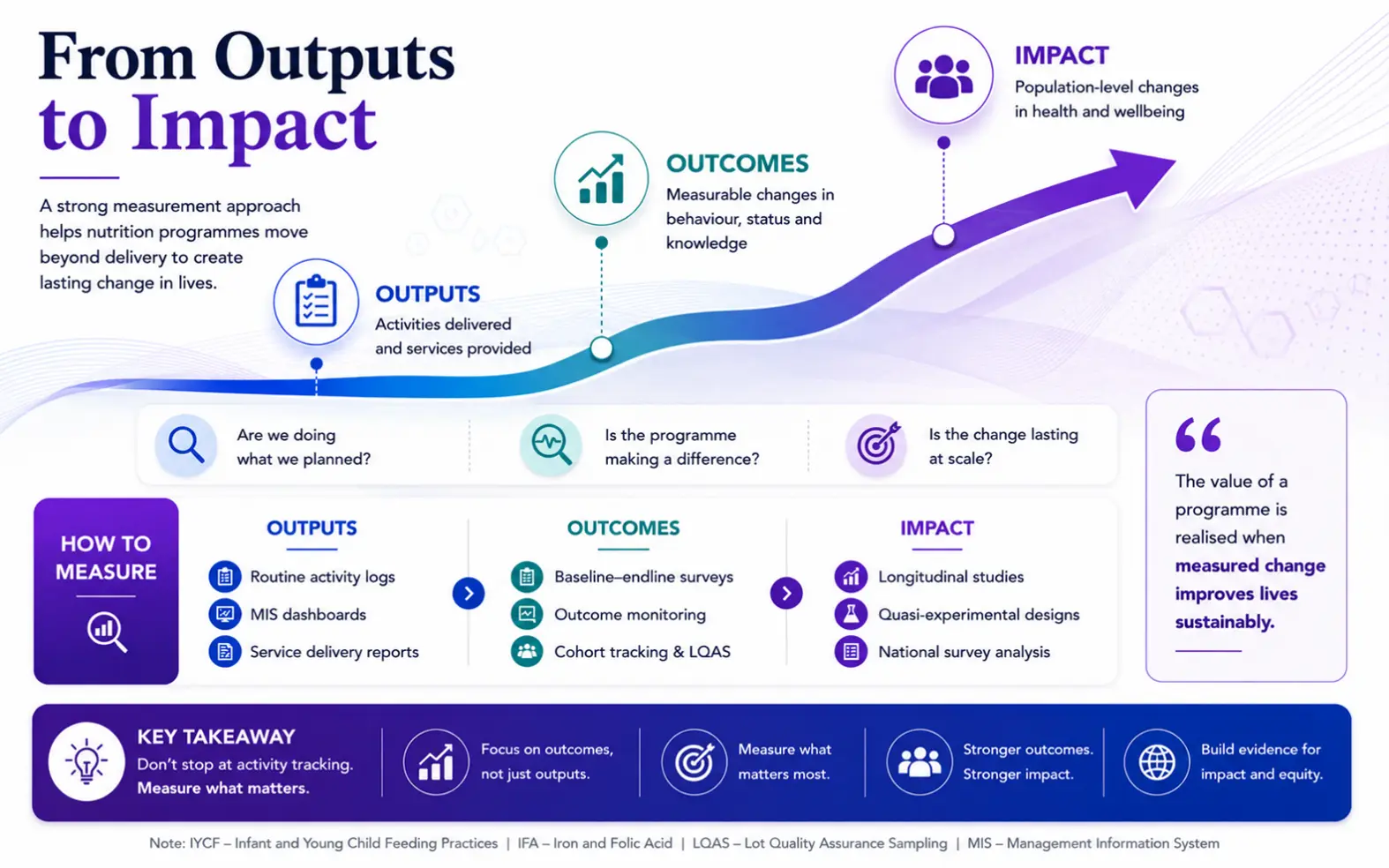
Figure 2: From Outputs to Impact– The Measurement Hierarchy for Nutrition Programmes.
Five Design Principles for Outcome-Driven Nutrition Interventions
Shifting from delivery-focused to outcome-focused programme design requires rethinking the architecture of the intervention– whether the setting is rural India, peri-urban Kenya, or conflict-affected Yemen. Five interconnected design decisions determine whether a programme produces measurable and sustainable nutrition outcomes.
1. Ground the Theory of Change in Local Evidence
A nutrition theory of change must articulate causal pathways between programme activities and the nutritional outcomes sought. It should specify what needs to change (dietary practices, care-seeking behaviour, micronutrient intake), in whom (pregnant women, adolescents, children under two), and through what mechanisms (counselling, community reinforcement, improved access, norm change). Critically, it must make assumptions explicit– untested assumptions are where programmes most often fail.
Across multi-location nutrition assessments, generic theories of change borrowed from other contexts rarely hold. A behaviour-change pathway effective in peri-urban Maharashtra may have limited relevance in tribal Jharkhand or pastoralist northern Kenya, where food systems, gender dynamics, and health access differ fundamentally.
2. Invest in Rigorous Baseline Research and Targeting
Evidence-based nutrition interventions require a strong diagnostic foundation. A well-designed nutrition baseline assessment goes beyond prevalence measurement to map dietary diversity, feeding practices, care-seeking patterns, intra-household food allocation, WASH access, and the social determinants that shape nutritional status– including women’s autonomy, household decision-making, and community norms around food and child-rearing.
This kind of baseline research serves multiple purposes. It enables precise geographic and demographic targeting, so that resources flow to where they will have the greatest effect. It establishes the reference point against which outcomes will later be measured. And it surfaces the contextual factors – often invisible in aggregate data – that will determine whether a given intervention succeeds or stalls.
3. Design Integrated Interventions, Not Isolated Activities
The evidence base is global and substantial: integrated nutrition programmes combining direct nutrition services with complementary actions in health, WASH, livelihoods, and behaviour change consistently outperform single-sector approaches. A programme distributing micronutrient supplements without addressing dietary practices, household food security, or complementary feeding quality is unlikely to produce sustainable nutrition outcomes.
Integrated nutrition programmes combine two types of actions. Nutrition-specific actions address direct causes: supplementation, fortified foods, growth monitoring and referral, counselling on infant and young child feeding practices. Nutrition-sensitive actions address upstream drivers: sanitation and hygiene, social protection, livelihood support, school-based nutrition education, and linkages to broader health services.
In several community-based interventions, the strongest outcome improvements emerge where nutrition counselling is paired with women’s group platforms, kitchen-garden support, and strengthened referral systems between community health centres and primary care facilities. Ethiopia’s Community-Based Nutrition programme, Rwanda’s community health worker model, and India’s Anganwadi-linked interventions each demonstrate that integration is about designing for the multiple pathways through which nutritional status actually improves.
4. Build Behaviour Change into the Core Design
Nutrition behaviour change remains among the most difficult outcomes to achieve and sustain. Feeding practices, dietary preferences, food preparation methods, and care-seeking behaviours are embedded in social norms, cultural identity, and household power dynamics. Generic awareness sessions delivered through lecture formats– still the default in many programmes across the Global South– rarely produce measurable change.
Effective nutrition behaviour change communication requires understanding specific barriers and facilitators at the community level and working through trusted local influencers– mothers-in-law, women’s self-help groups, community health workers, traditional birth attendants– who reinforce new practices within the social context where decisions are made. Programme timelines must acknowledge that behaviour change is iterative, slow, and non-linear. Short-term projects expecting rapid dietary shifts from brief exposure consistently disappoint.
5. Centre Maternal and Adolescent Nutrition Across the Lifecycle
The evidence linking maternal nutrition to child outcomes is unambiguous and universal. A mother’s nutritional status before and during pregnancy directly affects birth weight, early childhood growth, and long-term cognitive development. Adolescent nutrition shapes the nutritional reserves young women carry into their first pregnancies and influences intergenerational trajectories. Globally, exclusive breastfeeding rates rose from 37% in 2012 to 48% in 2023 (UNICEF Global Breastfeeding Scorecard 2024)– one of the few nutrition indicators showing sustained improvement– demonstrating that targeted, evidence-based programming can move the needle.
Yet many community nutrition interventions continue to focus primarily on children aged six months to five years, missing upstream determinants that begin well before birth. Outcome-driven programme design demands explicit attention to the full lifecycle– from adolescent girls through pregnancy, lactation, and early childhood– with indicators and service pathways designed for each stage.
Building a Nutrition MEL Framework That Drives Adaptive Programming
A robust monitoring, evaluation, and learning (MEL) framework is the operational backbone of any outcome-driven intervention. The distinction between a compliance-oriented M&E system and a genuine learning framework is significant. One counts and reports. The other generates insight, enables course correction, and builds the evidence base for future programming. An effective nutrition monitoring and evaluation system operates at three levels simultaneously.
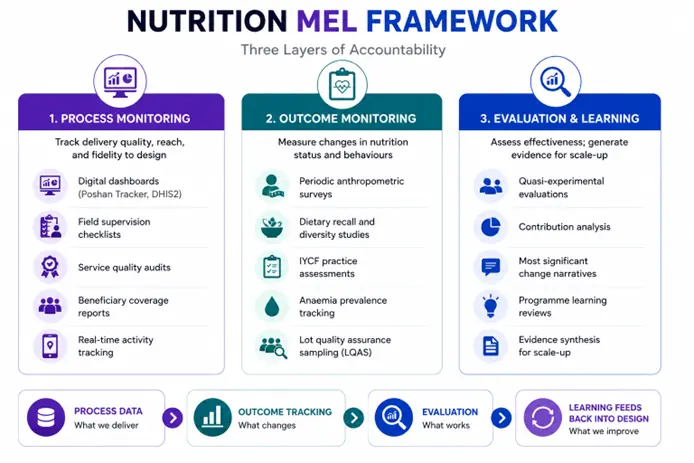
Figure 3: Nutrition MEL Framework– Three Layers of Accountability. Process data informs outcome tracking; outcome data drives evaluation; learning feeds back into design.
The Learning Loop: From Data to Decisions
Programme evaluations consistently reveal that the strongest-performing districts are not those with the best baseline indicators. They are the ones where supervisory structures review data monthly, frontline workers receive feedback on outcome trends rather than compliance scores, and programme managers have the authority and incentive to adapt.
Monitoring systems should not function only as reporting mechanisms. They should support programme learning and mid-course correction. If adherence is weak, the issue may be counselling quality. If attendance is low, the issue may be timing, accessibility, or trust. If outcomes vary by geography, the issue may be local context differences that a uniform delivery model cannot address.
The strongest programmes combine digital tools with direct observation, beneficiary feedback, qualitative interviews, and periodic validation. That triangulation matters because numbers alone rarely explain why one geography is progressing faster than another.
Digital nutrition tracking has advanced considerably. India’s Poshan Tracker, DHIS2 platforms across East and Southern Africa, and Bangladesh’s e-nutrition system all enable near-real-time data collection. But digital data alone does not produce adaptive management. The critical ingredient is the learning loop: the institutional discipline of reviewing data at regular intervals, identifying performance patterns, diagnosing bottlenecks, and making deliberate adjustments to delivery. Adaptive programming is a management discipline, not a slogan.
Sustainability: From Programme Dependency to Community Ownership

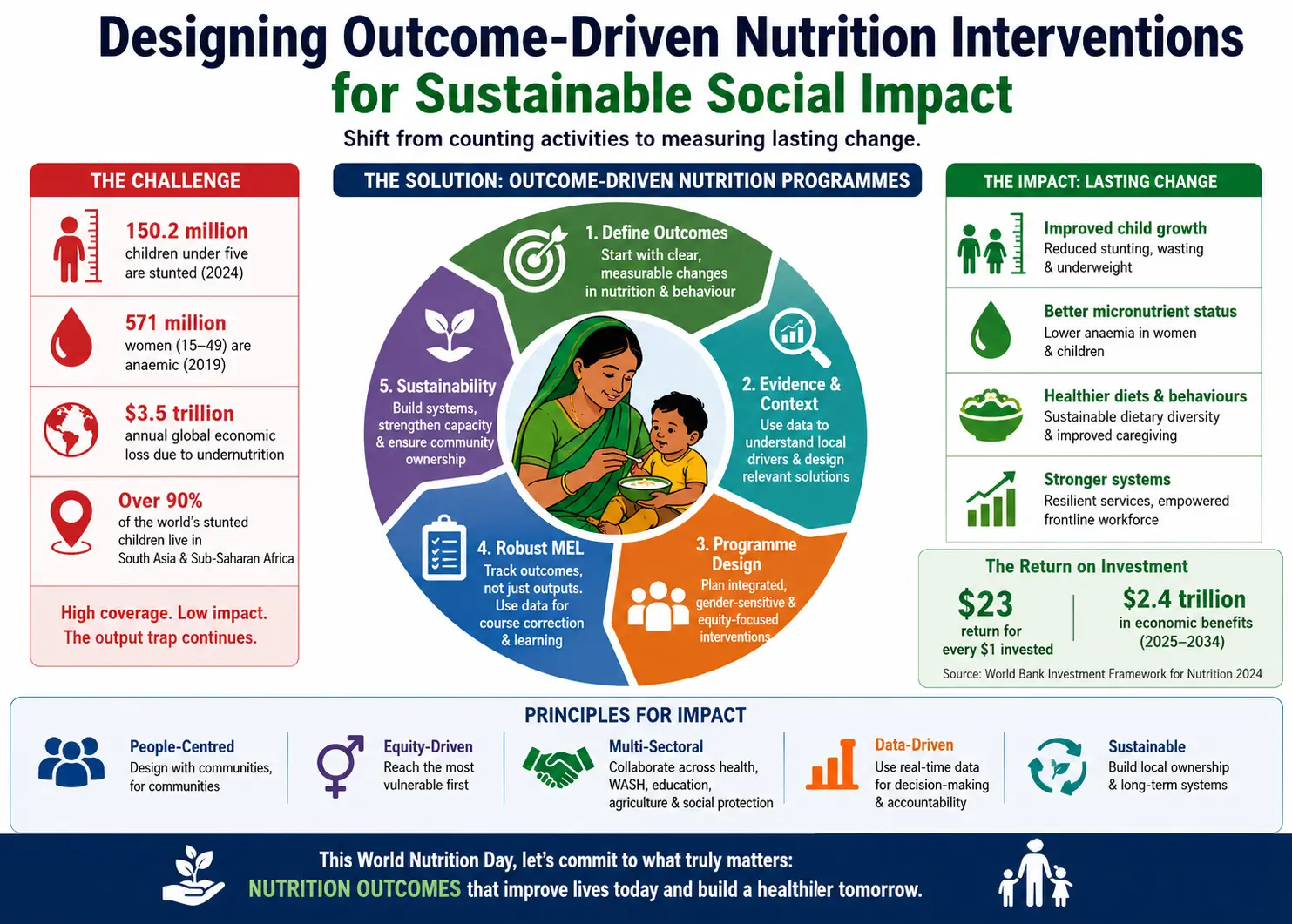
Figure 4: Outcome-Driven Nutrition Programme Lifecycle– Seven-Stage Design-to-Sustainability Framework with Continuous Learning Loop.
Programme sustainability is typically deferred to the final stages of a project cycle– treated as an afterthought rather than a design parameter. That is a fundamental mistake visible across contexts. Sustainable nutrition outcomes emerge from design decisions made at the outset, not from exit strategies drafted in the penultimate year. Three elements consistently distinguish programmes that produce lasting nutritional improvement from those where gains erode after external funding ends.
Local Institutional Strengthening
Nutrition interventions operating as parallel systems– staffed by project-funded personnel, governed by project-specific protocols– rarely outlast their funding. Programmes designed for sustainability work through existing institutions: Anganwadi centres and panchayat governance in India, community health extension systems in Ethiopia, health committees in Malawi, district health teams across francophone West Africa. The common principle is straightforward: invest in institutional capacity that outlives the project.
Community Ownership and Social Accountability
Lasting behaviour change is reinforced by community ownership– genuine agency in defining priorities, monitoring progress, and holding service providers accountable. Women’s groups, village health and nutrition committees, and community-based monitoring structures are not simply “participatory add-ons”; when well-designed, they become the durable architecture through which nutrition norms and practices are maintained.
Embedding Evidence in Institutional Decision-Making
Perhaps the most undervalued dimension of sustainability is the institutionalisation of evidence-based decision-making. When district-level teams are equipped to use their own data – to identify high-risk pockets, track outcome trends, and allocate resources accordingly – the dependency on external evaluations diminishes and the system becomes self-correcting. This is the long-term promise of investments in nutrition monitoring and evaluation infrastructure.
Strategic Recommendations for Funders, Designers, and Evaluators
The shift toward outcome-driven nutrition interventions is not abstract. It has concrete implications for how programmes are funded, designed, and evaluated. The following recommendations are drawn from accumulated field experience across community nutrition interventions, social impact evaluations, and multi-state programme assessments.
For Programme Funders and Donors
Fund baseline research as a non-negotiable component. Require theories of change that specify causal pathways and testable assumptions. Build longer programme timelines– nutrition outcomes, particularly stunting and anaemia reduction, require sustained effort over three to five years, not eighteen-month cycles. Invest in MEL systems that go beyond compliance reporting. The World Bank’s 2024 Investment Framework for Nutrition establishes that every $1 invested in evidence-based nutrition interventions returns approximately $23– making well-designed nutrition programming one of the highest-return development investments available.
For Programme Designers and Implementers
Resist the temptation to scale before the model is validated. Conduct formative research before finalising intervention design– in every new context. Integrate nutrition with complementary sectors from the outset. Train and support frontline workers as behaviour-change agents, not merely as commodity distributors. Build adaptive management into governance structures– regular learning reviews should be budgeted and calendared, not left to chance.
For Evaluators and MEL Professionals
Design evaluation frameworks that capture the full outputs-to-outcomes-to-impact chain. Use mixed-methods approaches combining quantitative rigour with qualitative depth– nutrition outcomes are shaped by social, cultural, and institutional factors that numbers alone cannot explain. Prioritise contribution analysis where randomised designs are infeasible. Feed evaluation findings back into programme design in real time, not only at the end of the cycle.
Social research support across the nutrition programme cycle
|
Programme need
|
Research support
|
Client value
|
|
Understanding the problem
|
Baseline studies, needs assessments and community diagnostics
|
Better targeting and clearer priorities
|
|
Designing the intervention
|
Change logic, targeting strategy and intervention model
|
Activities linked to desired outcomes
|
|
Tracking progress
|
MEL plans, indicator design, dashboards and field monitoring
|
Earlier course correction
|
|
Explaining results
|
Qualitative research, beneficiary feedback and case studies
|
Reasons behind the numbers
|
|
Measuring change
|
Midline, endline, impact evaluation and contribution analysis
|
Credible evidence of change
|
|
Planning scale
|
Scale readiness assessment and sustainability review
|
Lower risk before expansion
|
From Counting Meals to Measuring Change
World Nutrition Day should remind us that nutrition programming is not only about service delivery. It is about measurable improvement in health, behaviour, equity and wellbeing.
The path forward is not more programmes. It is better-designed programmes: grounded in local evidence, structured around clear outcome pathways, tracked through robust MEL frameworks, responsive to emerging data, and built for sustainability from day one.
World Nutrition Day is the right moment to ask whether nutrition programmes are truly fit for purpose. Not fit for reporting, not fit for visibility – but fit for the actual goal: improving the nutrition, health, and wellbeing of the people they serve.
Designing outcome-driven nutrition interventions is not about adding complexity. It is about adding clarity – to the target, to the logic, to the measurement, and to the plan for lasting change.
WORK WITH US
We partner with social impact organisations, development foundations, public health teams, NGOs, and CSR programmes to develop:
- evidence-based nutrition programme frameworks
- rigorous baseline assessments
- behaviour and social diagnostics
- adaptive MEL systems
- impact evaluations
- programme effectiveness studies
Get in touch to discuss your nutrition programme design, evaluation, or social research needs.
Sources and References
This article draws on data and evidence from the National Family Health Survey (NFHS-5, 2019–21), the UN State of Food Security and Nutrition in the World Report (2025), POSHAN Abhiyaan and Mission Poshan 2.0 programme documentation, the Poshan Tracker platform, WHO and UNICEF global nutrition monitoring data, and World Bank nutrition investment analyses. Observations on programme design and implementation are informed by the firm’s accumulated experience across nutrition assessments, baseline studies, programme evaluations, and social impact research engagements.













Share