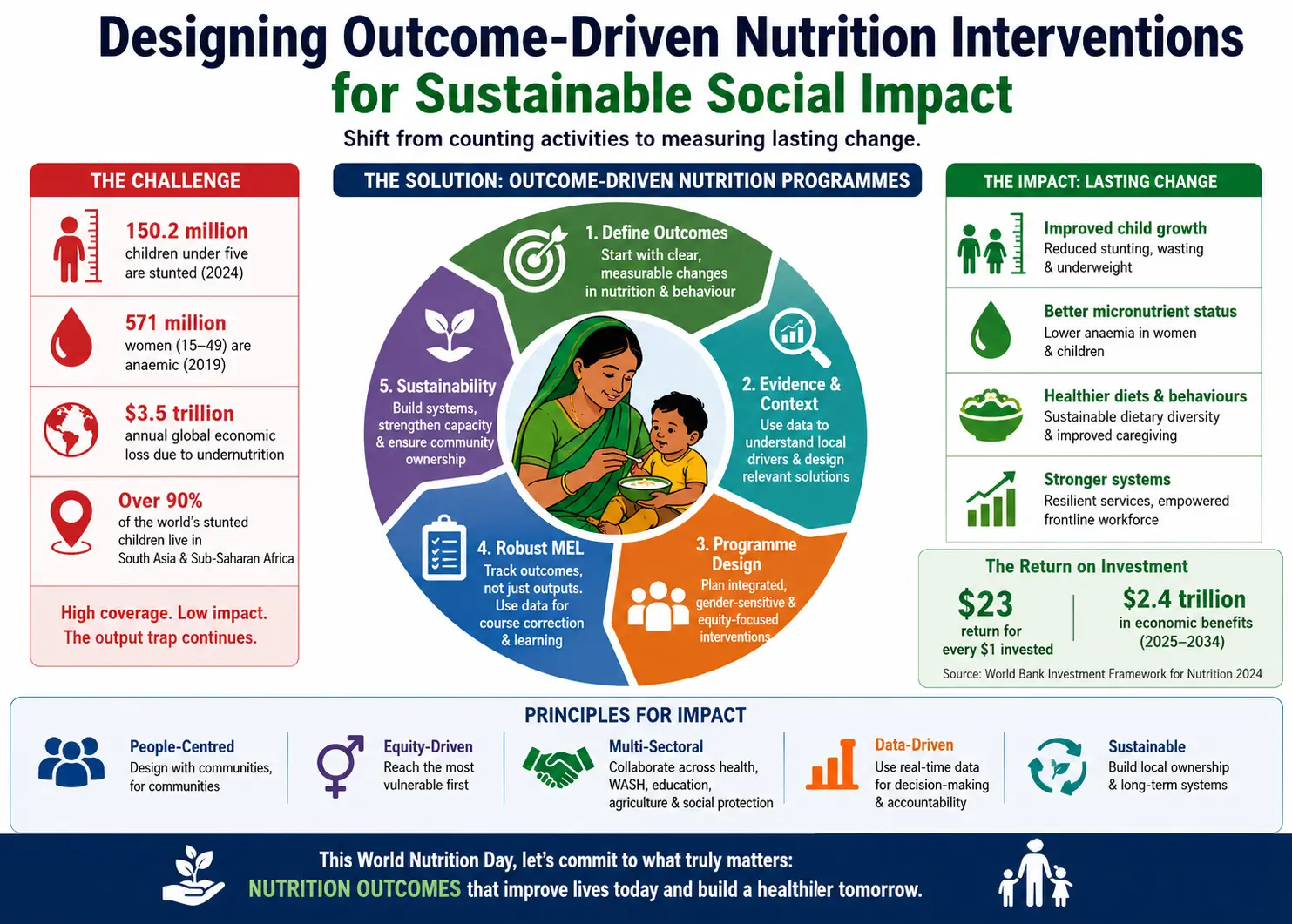
Drug-resistant refractory epilepsy (DRE) - defined as failure to achieve sustained seizure freedom after two appropriately chosen antiseizure medications - affects more than 17 million people worldwide, representing approximately one-third of all epilepsy patients. This case study demonstrates how Claight (Expert Market Research) delivered a comprehensive Drug-Resistant Refractory Epilepsy Epidemiology Forecast Report for 2018 to 2034 - covering 8 major markets across the US, Europe, Japan and India - that became a strategic planning tool for a global healthcare client navigating one of neurology's most complex and underserved disease areas.
|
17M+
DRE patients globally
|
~30%
of epilepsy patients
develop resistance
|
8
Major markets
modelled (8MM)
|
2018–2034
Historical + forecast
window
|
4×
Higher mortality vs.
general population
|
The Challenge: A Disease That Resists Treatment - and Resists Easy Quantification
Drug-resistant refractory epilepsy occupies a uniquely difficult position in neurology. By definition, it is characterised not by a specific pathology but by failure - the failure of two or more appropriately chosen and adequately dosed antiseizure medications (ASMs) to achieve sustained seizure control. This clinical reality, codified by the International League Against Epilepsy (ILAE), affects approximately 25–30% of all epilepsy patients globally - translating to more than 17 million individuals.
The clinical burden is severe and multidimensional. Beyond the physical toll of uncontrolled seizures, DRE carries a dramatically elevated risk of Sudden Unexpected Death in Epilepsy (SUDEP) - the leading cause of epilepsy-related premature death, predominantly affecting young adults. Individuals with DRE face an all-cause mortality rate approximately four times higher than the general population. Neuropsychiatric comorbidities - including depression, anxiety, and cognitive impairment - are pervasive, and the psychosocial consequences profoundly affect quality of life, employment, independence, and social participation.
Quantifying this burden with precision is not straightforward. Diagnosis is complicated by the phenomenon of pseudo-resistance: published studies indicate that 13–25% of patients referred for refractory epilepsy do not have true pharmacoresistance, with imitators including psychogenic non-epileptic events, misdiagnosed seizure type, and poor medication adherence. Without correcting for pseudo-resistance, patient population estimates are systematically overstated - a critical methodological issue with direct implications for commercial planning, trial feasibility, and healthcare resource allocation.
The Client: Navigating a Complex, Under-Quantified Disease Space
For a pharma or biotech company developing therapies in epilepsy, DRE represents both the highest unmet need and the hardest patient population to size with precision. Diagnosis is complicated by pseudo-resistance, and published epidemiological data across geographies vary significantly due to diagnostic infrastructure differences and registry gaps.
Our client - a pharmaceutical company with active assets across epilepsy and neurological disorders - faced a challenge that sits at the intersection of science and strategy: how to plan credibly in a disease area where the patient population is large, heterogeneous, and difficult to size with precision.
Three Linked Strategic Questions
Existing published epidemiology was fragmented, often outdated, and rarely stratified by the demographic and geographic dimensions the client needed. The engagement was structured around three specific intelligence gaps:
- How large is the DRE patient population - today and through the forecast horizon - across the US, the major European markets, Japan, and India, using a consistent, ILAE-aligned definition that excludes pseudo-resistance?
- How does the burden evolve by age group and gender across these markets, and which demographic segments will drive the greatest demand for specialist care, clinical trial enrolment, and long-term treatment?
- Where are the most significant unmet needs across the DRE care pathway - from diagnosis and referral through pharmacological optimisation, surgery evaluation, and neuromodulation - and which geographic markets combine the highest burden with the strongest infrastructure for evidence generation?
The fundamental challenge was not just knowing how many patients exist today - but understanding how that population will evolve through 2034, across eight very different healthcare systems and regulatory environments.
Our Approach: A Multi-Source, Country-Stratified Epidemiology Model
Claight built the Drug-Resistant Refractory Epilepsy Epidemiology Forecast Report (2018–2034) as a precision instrument for commercial and clinical planning - not a high-level disease overview. The model covered all eight major markets individually across prevalence, incidence, and mortality from 2018 through 2034, grounded in four analytical pillars:
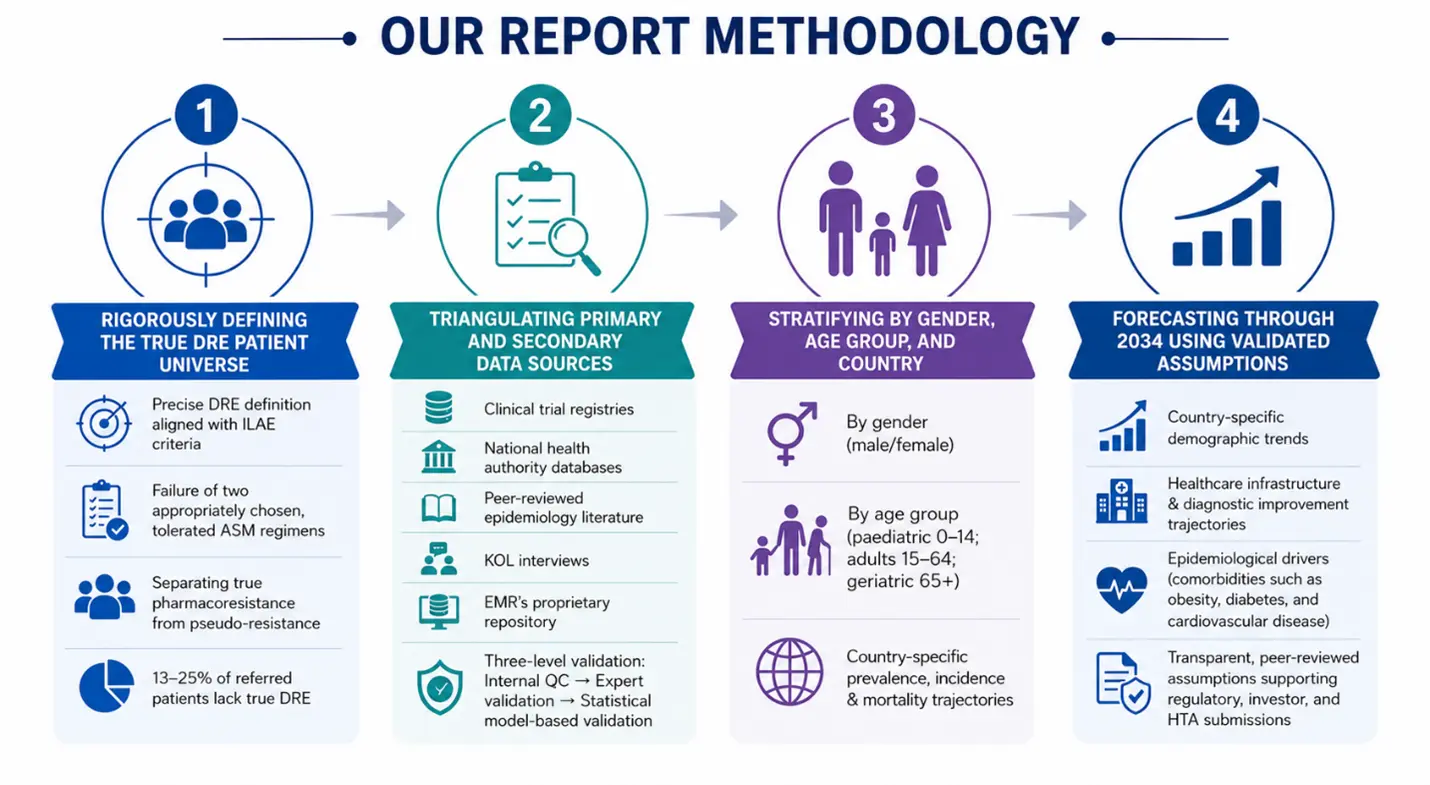
Pillar 1: Defining the true DRE patient universe
DRE was defined strictly using ILAE criteria: failure of two appropriately chosen, tolerated antiseizure medication (ASM) regimens. A key step was excluding pseudo‑resistance due to misdiagnosis, wrong ASM choice, under‑dosing, or poor adherence. Because 13–25% of “refractory epilepsy” referrals are not true DRE, removing them was essential to avoid overstating the addressable DRE population.
Pillar 2: Triangulating primary and secondary sources
DRE epidemiology data were drawn from clinical trial registries, government health databases, peer‑reviewed literature, national health authority reports, KOL interviews, and EMR’s proprietary data. A three‑step validation (internal QC, expert/KOL review, statistical checks) ensured each country estimate reflected real diagnostic practice and reporting, not just a global prevalence rate scaled to population.
Pillar 3: Stratifying by gender, age group and country
For every market, the DRE population was split by gender and age group (paediatric 0–14, adults 15–64, geriatric 65+). This allowed the client to see distinct patient pools for paediatric syndromes like Lennox‑Gastaut Syndrome versus adult focal epilepsy. Separate prevalence, incidence, and mortality curves were generated for each demographic stratum at country level.
Pillar 4: Forecasting through 2034 using validated assumptions
The DRE forecast to 2034 combined demographic trends (ageing in Europe and Japan, younger populations in India), changes in healthcare infrastructure, diagnostic improvement, and comorbidity drivers such as obesity, diabetes, and cardiovascular disease. Assumptions were documented and peer‑reviewed so the forecast could be used in regulatory dossiers, investor materials, and internal portfolio decisions.
Key Findings: What the 8MM Epidemiology Data Revealed
The model produced granular, validated epidemiology estimates for each major market from 2018 through 2034. The headline trajectory is unambiguous - the DRE burden is rising across all eight markets - but the strategic value came from the country-level patterns, demographic shifts, and market-specific dynamics beneath the aggregate numbers.
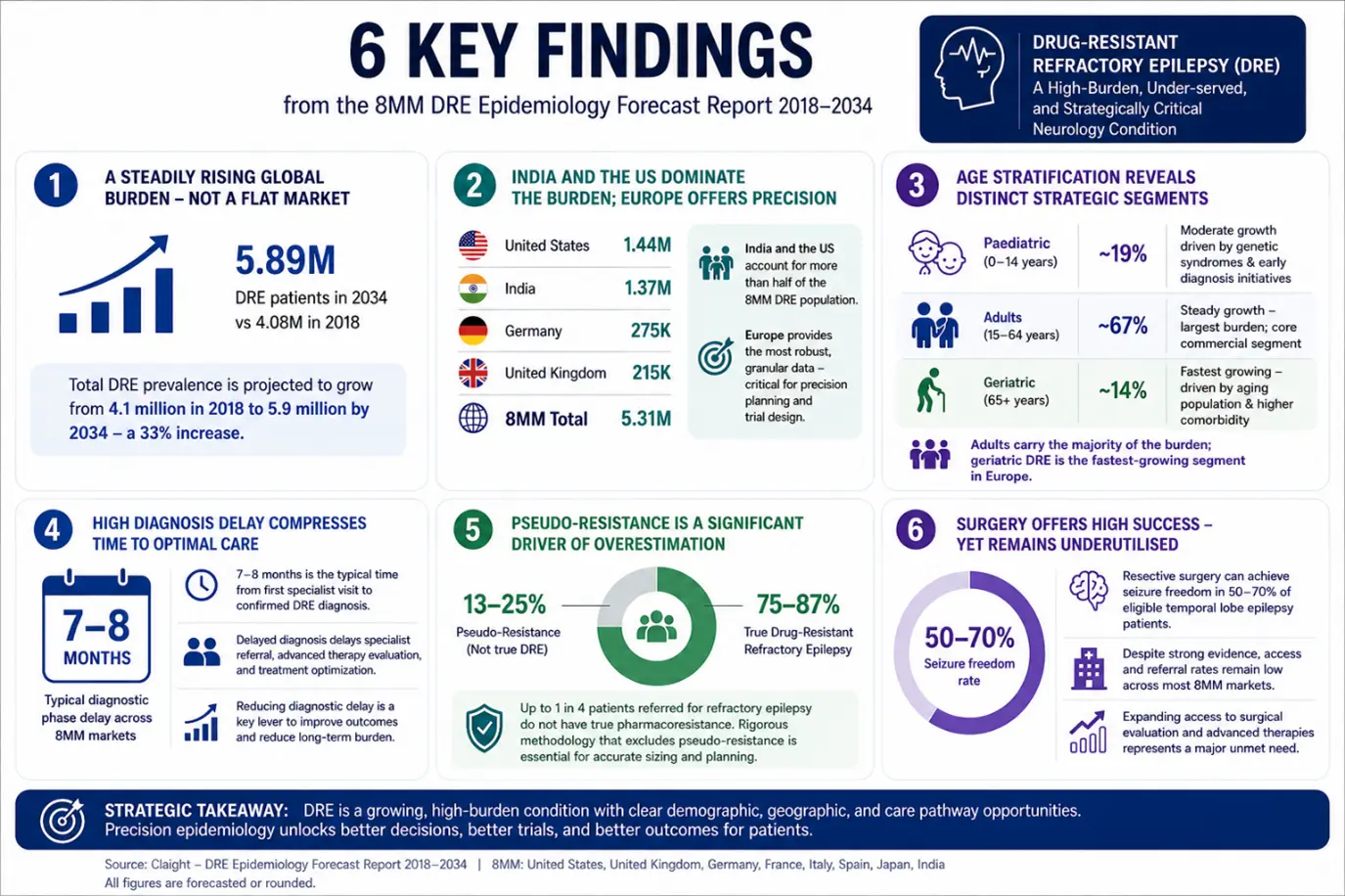
Finding 1: A Steadily Rising Global Burden - Not a Flat Market
Across the 8MM, total DRE prevalence is projected to grow from approximately 4.1 million in 2018 to 5.7 million by 2034 - a 39% increase. This trajectory is driven by a combination of population growth (particularly in India), ageing demographics in Europe and Japan, and improving diagnostic rates as healthcare infrastructure matures in emerging markets.
FIGURE 1: Total DRE Prevalence Across 8 Major Markets (2018–2034)
| Year |
8MM Prevalence |
Growth Trend → |
| 2018 |
4.08 million |
████████████████████████████████████████ |
| 2020 |
4.27 million |
█████████████████████████████████████████ |
| 2022 |
4.45 million |
███████████████████████████████████████████ |
| 2024 |
4.64 million |
█████████████████████████████████████████████ |
| 2025 |
4.75 million |
██████████████████████████████████████████████ |
| 2028 |
5.04 million |
█████████████████████████████████████████████████ |
| 2031 |
5.36 million |
████████████████████████████████████████████████████ |
| 2034 |
5.69 million |
███████████████████████████████████████████████████████ |
Source: Claight - DRE Epidemiology Forecast Report 2018–2034 | All figures are illustrative of trend direction; full data available in the report
Finding 2: Country-Level Prevalence: India and the US Dominate Burden
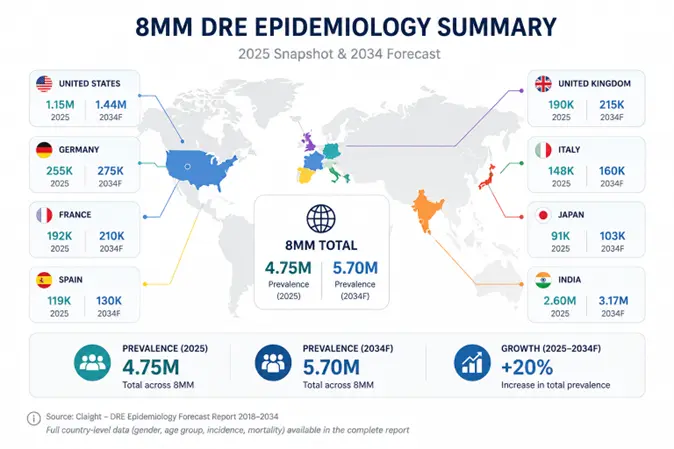
India accounts for more than half of the 8MM DRE population in absolute terms, driven primarily by population size and high unmet need - making it a critical market for any organisation with a global access strategy. However, epidemiological data for India require careful handling: significant underdiagnosis exists in lower-resource regions, and the report's modelling corrected for registry gaps using triangulated primary and secondary evidence.
The United States represents the largest developed-world market, with prevalence forecast to grow meaningfully through 2034. European markets - Germany, France, the UK, Italy, and Spain - are smaller in absolute volume but substantially better characterised, with mature diagnostic infrastructure, lower pseudo-resistance rates, and cleaner patient population data. This makes them priority markets for registrational trial sites, early commercial launches, and HTA submissions where credible patient counts directly influence reimbursement decisions.
FIGURE 2: DRE Prevalence by Country - 2025 Snapshot & 2034 Forecast
Finding 3: Age Stratification Reveals Distinct Strategic Segments
The age-stratified analysis produced findings with direct implications for trial design, patient access planning, and competitive positioning across the DRE market:
FIGURE 3: 8MM DRE Burden by Age Segment - Strategic Profile
| Age Group |
8MM Share |
Strategic Relevance |
Growth Outlook |
| Paediatric (0–14 years) |
~19% |
Dominated by severe syndrome-defined phenotypes (LGS, Dravet Syndrome); high DRE conversion rate |
Moderate |
| Adults (15–64 years) |
~67% |
Largest segment; highest absolute burden across all 8 major markets; core commercial population |
Steady |
| Geriatric (65+ years) |
~14% |
Fastest-growing segment in Europe (Germany, France, Italy, UK); new-onset epilepsy in older adults |
Fastest ↑ |
Source: Claight - DRE Epidemiology Forecast Report 2018–2034
The paediatric cohort warrants particular attention. In the UK, more than 90% of children diagnosed with Lennox-Gastaut Syndrome progress to DRE. In India, more than 60% of DRE patients had their first seizure before age 18. The paediatric DRE population is smaller in absolute numbers but highly concentrated in severe, syndrome-defined phenotypes - creating a distinct regulatory and commercial pathway with differentiated HTA expectations, separate from adult indications.
Finding 4: Female Predominance - with Clinical Consequences for Trial Design
Across most 8MM markets, adult women are slightly over-represented in DRE cohorts (52.6% female in the UK). Hormonal influences across the menstrual cycle, pregnancy and menopause affect both seizure frequency and ASM pharmacokinetics - making sex-stratified analysis essential for trial design and safety monitoring plans targeting women of reproductive age.
Finding 5: Mortality Patterns Diverge Meaningfully Across Markets
DRE carries approximately a 4× higher all-cause mortality risk versus the general population, with SUDEP representing the most acutely dangerous complication. However, mortality trajectories differ significantly across countries - a pattern with direct implications for the risk-benefit framing of new therapies and the evidence bar payers in each market expect.
- In Germany and Italy, absolute DRE mortality is tracking slightly downward through the forecast period - consistent with improving standard of care and stronger specialist referral pathways.
- In the US and India, mortality rises in line with prevalence growth - indicating that improvements in care are not yet outpacing the expanding disease burden.
- These diverging trends affect how regulators and payers in each market will evaluate comparative benefit, particularly for therapies targeting high-risk populations such as SUDEP-prone patients or those with severe comorbidities.
Finding 6: Treatment Gaps and Unmet Needs Persist Across All Eight Markets
The report's patient journey and unmet need analysis identified structural gaps in DRE care that remain consistent across geographies, creating persistent commercial white space for innovation:
- Diagnosis: 7–8 month average delay from first seizure to DRE confirmation; specialist referral often late
- Surgery: 50–70% seizure-freedom rate in eligible patients, yet temporal lobectomy volumes remain flat
- Neuromodulation: RNS use grew significantly from 2012 to 2019 but penetration vs eligible population stays low
- Comorbidities: psychiatric disorders prevalent in DRE yet systematically underscreened and undertreated
Strategic Impact: Turning Fragmented Estimates Into a Coherent DRE Strategy
The Drug-Resistant Refractory Epilepsy Epidemiology Forecast 2018–2034 gave the client a single, validated, country-stratified evidence base for decisions that had previously relied on inconsistent published estimates or internal assumptions. The impact was felt across four strategic functions:
01. Commercial Planning & Market Sizing
- Consistent ILAE-aligned population sizing across all 8 markets simultaneously
- Revenue modelling and launch sequencing underpinned by validated patient counts
- Payer engagement strategies anchored in data - not extrapolated global averages
↳ Credible country-by-country commercial baseline for the DRE portfolio
02. Clinical Trial Design & Enrolment Planning
- Country-level incidence data drove site selection and screen-failure rate modelling
- Age-stratified targets set separately for paediatric and adult enrolment cohorts
- Gender split findings shaped safety monitoring protocols for women of reproductive age
↳ Enrolment feasibility grounded in real, stratified patient counts - by market
03. Portfolio Prioritisation - US & European Markets
- Germany and France identified as priority EU launch markets based on stable adult DRE trajectory
- UK paediatric DRE profile shaped a differentiated go-to-market strategy for syndromic assets
- 2034 forecast modelled the patient pool at the anticipated time of market authorisation
↳ Country sequencing decisions supported by a 10-year patient trajectory - not a point estimate
04. Regulatory & HTA Submissions
- Three-level validated data ready for FDA, EMA, NICE, G-BA (AMNOG), and HAS (ASMR)
- Peer-reviewed methodology defensible in regulatory meetings and reimbursement dossiers
- Patient population estimates - not market size proxies - supported payer pricing discussions
↳ Single evidence base spanning trial design, regulatory submission, and commercial launch
Country-level DRE prevalence and mortality data, stratified by age and gender and validated through a rigorous three-level protocol, gave our client a foundation for decisions that go all the way from trial site selection to pricing discussions with European payers.
This is the difference between epidemiology as a background fact and epidemiology as a strategic instrument.
Read more about our Epidemiology forecasting services here
Why Epidemiology Forecasting Matters in DRE and Beyond
Epidemiology forecasting in DRE is useful only when it helps answer the real questions teams face. Because DRE is hard to diagnose, varies by geography, and differs by age, gender, and syndrome, a single global prevalence number is not enough. Biopharma teams need a clear, forward-looking view of the patient population that speaks directly to development, launch, and market access decisions.
Claight’s country-level disease burden modelling is built to answer questions such as:
- Where is the addressable patient population growing fastest, and at what rate, across my priority markets?
- Which patient segments (age, gender, syndrome) are most relevant for my asset, and how large are they today vs at expected launch?
- What does this mean for clinical trial design - site selection, expected screen failure rates, and realistic enrolment timelines?
- How do severity and mortality trajectories differ between early-launch European markets and those planned for later access?
- What epidemiology evidence will regulators and payers (FDA, EMA, HTA bodies in the UK, Germany, France) expect, and does my current data package meet that bar?
- How sensitive are my opportunity and revenue forecasts to key assumptions such as diagnosis rates, treatment patterns, and demographic change?
While this case study focuses on Drug-Resistant Refractory Epilepsy, the same question-led approach and modelling framework apply to other complex areas - including rare and orphan neurological diseases, cardiometabolic and respiratory conditions, oncology indications, and paediatric diseases where precise patient population sizing and stratification are critical for regulatory and commercial success.
Also take a look at our Drug-Resistant Refractory Epilepsy Pipeline Insight 2026 Report
How Claight Supports Strategic Healthcare Intelligence Globally
Claight (Expert Market Research) delivers customised healthcare market intelligence and strategic research solutions across pharmaceuticals, biotechnology, diagnostics, medical devices, and healthcare services. Our work combines rigorous epidemiology modelling, competitive intelligence, drug pipeline analysis, and therapeutic landscape assessment to support evidence-based decision-making across the full product lifecycle - from early development through to market launch and lifecycle management.
We support global clients across North America, Europe, Asia-Pacific, and emerging markets, including pharmaceutical companies, biotechs, healthcare investors, payers, regulatory organisations, and policy institutions.
Click here know more about our Healthcare Intelligence Services
Ready to Build Your Neurological Disease Epidemiology Model?
Whether you need a full 8MM epidemiology forecast, a single-country deep dive, a syndrome-specific patient sizing model, or a pipeline-to-patient market readiness assessment, Claight can build it - validated, stratified, and ready for regulatory and commercial use.
Contact us: sales@expertmarketresearch.com
Visit: www.expertmarketresearch.com
Our team supports engagements across drug pipeline analysis, epidemiology forecasting, market sizing, competitive intelligence, and regulatory strategy - globally.













Share